|
TOTAL KNEE REPLACEMENT
A Guide for Patients
Basford Consulting Rooms has a number of Orthopaedic Surgeons who specialise in Knee Replacement Surgery.
Introduction
This leaflet provides information for you and your family regarding total knee replacement. Your Consultant may recommend a total knee replacement for you, but the decision to have the operation is yours. Your decision must be based upon weighing the benefits against any risks. If you have any questions as you read through this leaflet then ask the Consultant, nurse or therapist at your next visit. You may find it helpful to make a note of your questions before you see the Consultant or nurse.
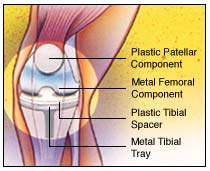
What Is a Knee Replacement?
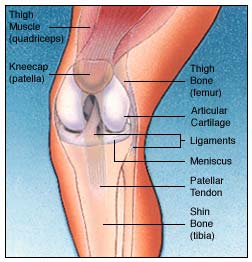 Total Knee Replacement is a surgical procedure in which damaged parts of the knee joint are replaced with an artificial joint (prosthesis). During the procedure the worn out surfaces of the femur and tibia are removed and replaced with smooth artificial surfaces and a plastic insert between them. The knee cap (patella) may or may not be resurfaced with another piece of plastic. These artificial pieces are attached to the bone with bone cement (methyl-methacrylate) or special coatings, which encourage the bone to grow onto the prosthesis. Your Consultant will decide which is suitable for you. Total Knee Replacement is a surgical procedure in which damaged parts of the knee joint are replaced with an artificial joint (prosthesis). During the procedure the worn out surfaces of the femur and tibia are removed and replaced with smooth artificial surfaces and a plastic insert between them. The knee cap (patella) may or may not be resurfaced with another piece of plastic. These artificial pieces are attached to the bone with bone cement (methyl-methacrylate) or special coatings, which encourage the bone to grow onto the prosthesis. Your Consultant will decide which is suitable for you.
An artificial knee is not as good as a normal knee, but by replacing your diseased knee joint with an artificial joint, knee replacement surgery can relieve your pain and help you to get back to enjoying normal, everyday activities again.
Why Have A Knee Replacement?
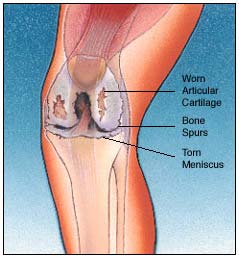 Osteoarthritis is the most common reason for a knee replacement. Osteoarthritis is a degenerative disorder often referred to as wear and tear arthritis. Osteoarthritis is the most common reason for a knee replacement. Osteoarthritis is a degenerative disorder often referred to as wear and tear arthritis.
However, there are many other types of arthritis such as rheumatoid arthritis, which is caused by inflammation in the joint.
You may benefit from knee replacement if: 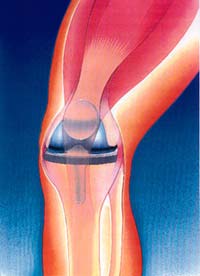
· You have daily pain preventing you from walking any distance or going up and down stairs
· The pain is moderately severe at rest or wakes you at night
· Your joint movement becomes limited by stiffness
· Your knee constantly gives way
· Your knee is becoming very bowed or there is significant swelling that does not improve with rest.
Although most patients who undergo knee replacement are over 60 years of age, recommendations for surgery are based on the amount of disability rather than age.
Your consultant will often try simple conservative measures to control your pain before opting for surgery such as pain killers, anti-inflammatory tablets, weight loss and physiotherapy. When your arthritis becomes so severe that medication, reducing your level of activity and using walking aids are no longer helping, you may want to consider a knee replacement.
How Successful Is A Total Knee Replacement?
Results are normally very good. Almost all patients are relieved of their knee pain. As the pain lessens, function also improves.
An artificial knee is not a normal knee and it will not allow you to return to active sports or heavy manual work. Activities must be avoided that overload the artificial knee. Most patients have an improved range of movements and limp less, but 5-10% of patients continue to have stiffness.
How Long Do Total Knee Replacements Last?
 Knee replacements do eventually wear out. Wear is the major long-term problem but 90% of total knee replacement joints will last for 10 years or more Knee replacements do eventually wear out. Wear is the major long-term problem but 90% of total knee replacement joints will last for 10 years or more
When a knee replacement does wear out it can be revised. The results of a second operation (revised knee) are not as good as the first time around. This is why your doctor will often try other forms of treatment first.
Wear of the knee replacement is in part related to your weight and activity. After your operation it is important to control your weight and avoid excessive amounts of exercise such as jogging, contact sports, skiing or weight lifting. You are also at risk of the knee joint loosening if you have osteoporosis.
Are There Any Risks Involved?
Yes, a knee replacement is a major operation. The health team looking after you will try to make your operation as safe as possible. However, in every procedure there is a risk of complications. Some of these can be serious or very rarely even cause death. The possible complications of this operation are listed below. Please ask your doctor if there is anything you do not understand. Any risk numbers given are from reliable studies of patients having this operation. Your doctor may be able to tell you if the risk of a complication is higher or lower in your particular case.
The complications specific to a total knee replacement fall into three categories: complications of anaesthesia, complications of any operation and complications specific to having a knee replacement.
· Anaesthetic risk.
You will be seen in the assessment clinic for health screening to try to make you as fit as possible for your operation. There is a risk of 1 in 350 of a heart attack following knee replacement and also a risk of stroke and chest infections. Your anaesthetist will also see you before your operation to discuss the risks and the anaesthetic choices available.
The choices are general anaesthetic, spinal anaesthetic or a combination of these. Your anaesthetist will be able to advise you of which technique might be more suitable for you, taking into account your general health.
The anaesthetist will also advise you of any other special techniques, which might be necessary for you and give you an indication of any particular risks regarding your general state of health.
· Bleeding
You will be asked to attend for a blood test within 5 days of your operation in case you need a transfusion during or after the operation.
· Infection
Infection in the surgical wound can be a complication of any operation. Usually these clear up quickly with antibiotics. There is also a risk of 1 in 50 of the new knee becoming loose or failing over a period of a few months due to infection. If this happens you will need one or more further operations to control the infection. Some infections like MRSA are resistant to common antibiotics and therefore are more difficult to treat. At the Preoperative Assessment we screen for MRSA by taking swabs from the nose and perineum of all patients coming in for joint replacement surgery.
MRSA can be treated before admission. To reduce the risk of infection the theatres are equipped with a special filtered ventilation system; you will be given antibiotics intravenously while you are under the anaesthetic and all the wards have alcohol gel dispensers to help provide better hand hygiene and prevent cross-infection between patients.
· Scarring
There will be a scar on the front of your knee, which is usually very neat and will fade over time.
· Deep vein thrombosis or DVT.
This is a blood clot in the veins of your leg. Occasionally the clot can dislodge and travel to the lungs (pulmonary embolus). The risk of thrombosis is 1 in 11 and the risk of an embolus is 1 in 2,000. To help avoid thrombosis the physiotherapists and nurses will get you moving around as soon as possible, usually on the day after your surgery. You will be given blood-thinning medication to prevent blood clots forming and you will also be fitted with special elastic anti-embolism stockings on admission. These help increase the blood flow in your legs and they are usually worn for six weeks after surgery.
· Retention of Urine
Difficulty passing urine may occur, which might mean you needing a catheter to drain your bladder for a day or two.
· Chest infection.
If this happens you may need a course of antibiotics and physiotherapy.
· Heart attack or stroke
This can happen after any major operation. The risk of a heart attack is 1 in 350 and either complication can occasionally be fatal.
· Nerve injury.
There is a 1 in 170 risk that the nerves that run behind the knee joint may be damaged during the operation. If nerve damage did occur it would lead to weakness, numbness or pain in the leg or foot.
· Loosening.
The risk of loosening occurring without infection is 1 in 40 in the first 10 years after the operation.
· Stiffness.
Sometimes your new knee remains very stiff after the operation and it may be necessary to give you another light anaesthetic so that the knee can be manipulated while you are asleep to loosen it up.
· Bruising and swelling.
It is normal for significant bruising and swelling to occur after the operation, which can sometimes take several weeks to go down.
· Damage to blood vessels.
There is a risk of 1 in 650 of damage to the blood vessels behind the knee, leading to loss of circulation to the leg and foot. If this happens you will need immediate surgery to restore the blood flow.
Getting Ready For Your Operation
It is important that you are fit for your operation as you will make a quicker recovery.
If you smoke, try to cut down or quit, ideally 8 weeks or more before your operation. Smoking changes blood flow patterns, delays healing and slows recovery. Even stopping for 24 hours before the operation is beneficial. If you want to stop smoking ask for information about the Smoking Cessation Nurse or talk to your General Practitioner or Practice Nurse.
Keep your weight down. Being very overweight (i.e. a Body Mass Index of greater than 30) can significantly increase the risk of complications from surgery and anaesthesia, make the operation more difficult and reduce the life of your knee replacement. The assessment nurse will weigh you and measure your height and give you some advice. You may find it helpful to talk to your General Practitioner or Practice Nurse. If you are seriously overweight your consultant may delay surgery until you have lost some weight.
Have a dental check if you have not done so in the last six months. It is important that any dental infections are dealt with before joint replacement surgery to prevent infection in your new knee. If infection is suspected your operation will be postponed.
Start some gentle exercises according to advice from your doctor or physiotherapist. These may be uncomfortable at first but persevere, as exercises help the muscles around the joints become stronger and reduce stiffness. They will also aid your recovery following surgery.
Being as fit as possible before the operation will speed recovery and reduce the risk of complications. It is worth trying to walk a short distance each day as pain permits, or take up gentle exercise such as swimming to improve your level of fitness and mobility. Activities which improve upper limb strength will improve your ability to use walking aids after the operation.
The new knee joint needs strong muscles to keep it stable, so if possible it is a good idea to do some exercises at home before the operation. It has been found that patients who do this at least once or twice a day consistently (as pain permits) make a quicker recovery and find rehabilitation easier.
Quadriceps Set
The quadriceps is the front knee muscle. Tighten this muscle to make your kneecap move hold this contraction for 5 counts and then relax. This exercise is done with the leg straight and can be performed standing, sitting or lying down.
Straight Leg Raise
Lie on your back with opposite knee bent. Tighten the knee muscle performing a quad set. Lift your straight
leg up slightly to just lower than your bent knee and hold for 3-5 counts. The knee should be straight
throughout the lift. Relax leg between each lift.
Terminal Knee Extension
Lie on your back and place towel roll under your knee allowing your knee to bend slightly. Lift heel in order to straighten your leg. Hold for a count of 5 and then relax.
Lying or sitting on bed bend your knee up by taking your heel towards your bottom, bend your knee as far as you can and then straighten your knee.
Sitting in a chair or on a bed bend your knee as far as you can and then straighten your knee out, hold for a count of 5.
Lying on your tummy bend your knee up behind you taking your heel towards your bottom.
Before Your Operation
Knee Education Group
 You may be asked to attend an education session about all aspects of your operation, hospital stay and recovery, which lasts about an hour and a half on a Wednesday afternoon. You can bring someone with you if your wish. You may be asked to attend an education session about all aspects of your operation, hospital stay and recovery, which lasts about an hour and a half on a Wednesday afternoon. You can bring someone with you if your wish.
You will meet one of the Pre-operative Assessment Nurses, a Physiotherapist and a member of the Occupational Therapy team, and have a chance to ask them questions.
Pre-operative Assessment
A few weeks before your operation you will be asked to attend a preoperative assessment clinic where you will undergo routine investigations such as blood pressure measurement, blood tests and heart tracing (ECG).
Please bring your tablets, inhalers and any other medicines you take. If you take medicine for high blood pressure it would be helpful to bring some recent blood pressure readings. If you are diabetic please bring a record of your blood sugar readings. If you are on Warfarin please bring your yellow book.
If you are unable to keep your appointment for admission or for preoperative assessment please inform us as soon as possible using the contact numbers at the back of this booklet. Late cancellations waste operating time and lengthen the waiting list.
Plan Ahead For Your Homecoming
Getting the full benefit from knee replacement surgery can take a few months and during this time a full range of movement may be difficult. As a consequence many people find they are limited in their ability to do normal activities such as bathing, shopping, laundry, cooking and housework. Help from others may be needed.
It is important to plan ahead and think about the support you will need when you go home, usually at around three days after surgery.
Here are some suggestions to start thinking about:
· Arrange for someone to take you home from the hospital. You will not be allowed to drive for six weeks after your operation.
· If you are caring for someone else you will need to make alternative arrangements for their care (respite, home care, help from friends or family)
· Is anyone available to help you when you come out of hospital? It is better if someone can be with you for the first week or two following discharge to help with things like cooking and personal care, if only for part of the day. If you do have any concerns about going home please discuss them with the Assessment Nurse.
· It is a good idea to prepare and freeze some meals in advance or arrange for relatives and friends to bring meals.
· Organise your kitchen to avoid excessive lifting and bending. The Occupational Therapist can advise you on the use of equipment to assist you in the kitchen.
· Remove any rugs that could cause you to trip. Securely fasten any electric wires and ensure a safe passage throughout your home.
Will I Need Anything Special At Home?
 The Occupational Therapist (OT) will assess your requirements and prescribe and order any appropriate equipment to help The Occupational Therapist (OT) will assess your requirements and prescribe and order any appropriate equipment to help  
you once you are back home. You will be asked to provide information about your home environment and how you are
coping at home prior to your admission, usually at the Pre-operative Assessment Clinic. The Occupational Therapist will
show you how to carry out activities of daily living safely. They will also discuss managing everyday activities safely after
knee surgery.
You will require a suitable armchair. The Occupational Therapist will advise you on the height of the chair. It must not be
too low, soft or deep. You should be able to get out of the chair easily without bending your knee at more than a right angle.
Chairs without arms should be avoided initially. Swivel office chairs and manually reclining chairs are not recommended.
Depending on the height of your toilet seat you may require a raised toilet seat for at least 6 weeks
When Will I Be Admitted To Hospital?
Usually you will be admitted to the Ward on the day of your operation.
Please only bring on admission what you will need for the first couple of days such as medication, toiletries, nightwear, glasses etc.
Before you go to theatre:
A member of the medical team will mark the limb to be operated on
Your anaesthetist will meet you and discuss the types of anaesthetic and pain relief available
It is essential that you do not have anything to eat, drink or chew for some hours before your operation, as this could cause vomiting while you are under the anaesthetic
You will have a shower and change into a hospital gown. You will be asked to remove any make-up or nail polish and all jewellery except for a wedding ring.
You will be transported to theatre in your hospital bed.
What to Expect After Surgery
After surgery you will be monitored closely while you wake up from your anaesthetic. When you are awake you may go to the Extended Recovery Bay.
Every effort is made to ensure your comfort and safety. This means that you will have your blood pressure, heart rate and oxygen levels monitored throughout. You will have a drip in your arm to ensure you get enough fluids. You will be able to have a drink a few hours after your operation has finished providing that you do not feel sick. If sickness is a problem, anti-sickness medicine will be given to you. You will be able to eat as soon as you feel like it.
You will have drainage tubes in your wound to prevent any bruise forming and to collect any blood loss. Sometimes this blood loss is collected, cleansed - with a machine called a Cell Saver - and re-infused to you through the drip. Some patients require a blood transfusion. You will be given oxygen through a mask for a few hours.
It is recommended that you bring a small overnight bag containing toiletries into hospital to take with you to the Recovery.
Pain Management
Some discomfort or pain after surgery is normal. The nursing staff will assist you to control any pain through injections or tablets.
Your anaesthetist will discuss the best method of controlling your pain with you.
There is a form of pain relief available called a PCA (Patient Controlled Analgesia). This means you will have a pump, which you control yourself to administer small doses of pain-killer by pressing a button on the handset whenever you need more pain relief. It is very safe and you will be closely monitored by nursing staff.
Another form of pain relief is an epidural. The anaesthetist inserts a thin hollow needle into the epidural space, just outside the outer covering of the spinal cord in the lower back. A small plastic tube is then introduced through the needle and left in position when the needle is removed. The tube is used to introduce local anaesthetic and pain killing medication. An epidural provides pain relief for as long as it remains in place, usually overnight. It may cause some temporary numbness and weakness in the legs, which wears off after three or four hours.
The nursing staff will assess you regularly to find out how comfortable you are. Suffering from pain can slow down recovery, so please tell the nursing staff if you are in pain at any time. While the pain may be acceptable when you are resting, it will increase when you move, and it is important to change position regularly and do exercises 5-6 times a day following the operation, so it is important to take pain relief regularly. We will be happy to help you in any way to make your stay as comfortable as possible.
On the first day after your operation you will be shown how to Straight Leg Raise by your Physiotherapist. When you are able to do this, they will show you how to get out of bed. They will also show you the correct way to move safely. You will also be shown exercises to regain movement and strength in your knee. You will be expected to carry out your own exercises and practice walking once the Physiotherapist decides it is safe for you to do so.
Knee Splints

Your Consultant may or may not want you to wear a knee splint to keep your knee straight until you can Straight Leg Raise.
How Your Knee Will Feel Different
Some numbness in the skin around the wound area is common and may improve with time. Kneeling is usually uncomfortable after a knee replacement and you will not be able to sit back on your heels. Occasionally, you may feel some clicking when walking or bending the knee. Your new knee may activate metal detectors at airports, so tell the security guard about your knee replacement if the alarm goes off.
Dos And Donts after Surgery
Everyone heals at different rates, so you may find you are able to carry out some activities fairly quickly following your operation. Provided this does not cause any pain or discomfort you can continue with caution.
Remember if an activity causes you pain STOP- its obvious your new knee is not ready yet
DO:
· Carry on with the exercises as instructed by your physiotherapist
· Take regular short walks
· Keep walking with your walking frame until the physiotherapist says you are safe to progress to elbow crutches or 2 walking sticks. 
· Stand and sit as shown in hospital operated leg in front, push on the arms of the chair, bed mattress or toilet seat frame
· Avoid pressure on the wound until it has fully healed and keep the wound dry until the skin has fully healed
· Go to your GP if you have an unusual pain, temperature, notice a discharge from your wound or any pain or swelling in your calves
· Please return any sticks or equipment when you have finished with them
· Ensure you take regular pain-killers for as long as you need to
· Eat a balanced diet with plenty of fresh fruit and vegetables
DONT:   
· Cross your legs, knees or ankles
· Sit on low chairs, stools or toilets
· Drive a vehicle until advised it is safe to do so. Usually this is after 6 weeks if you can
sit comfortably in your car and perform an emergency stop safely.
· Do any heavy lifting, housework or gardening
· Discard any walking aids until advised to do so
· Do too much too soon gradually increase your activities as able.
· Return to work or sporting activities until advised to do so
· Try to get into a bath or shower for the first 6 weeks because of the risk of falling
Community Intermediate Care
The Community Intermediate Care Team is a team of Qualified Nurses, Health Care Support Workers and Therapists who can support your early discharge home following your knee replacement.
The Community Intermediate Care Team can support the early transfer of care from hospital to your own home, for a period of recovery, recuperation and rehabilitation. They will provide the most appropriate care package for you, tailored to your individual needs, for up to 7 days.
With your initial consent, a co-ordinator will visit you at home between your pre-operative assessment and your date of admission to discuss the service with you and gain your agreement for supported early discharge.
The team also works very closely with other colleagues in the community, such as District Nursing teams and Social Services and will liaise with these services if you require ongoing care and support in your own home.
When You Go Home
It is important to continue with your exercises. The success of the operation has a lot to do with how well you do your exercises and strengthen your muscles. This part of your recovery is very much down to you.
If excess muscle aching occurs, cut back on your exercises but do not stop.
Wound stitches or staples are removed on about the twelfth day after surgery. The Community Intermediate Care Team will arrange for a District Nurse to visit you in your own home.
Bathing
It is recommended that you do not get into the bath for at least 6 weeks following your knee replacement as this can put excessive strain on the new joint.

A strip wash is recommended or you may use a walk-in shower with assistance once your stitches have been removed, as long as there are no steps into the shower.
Using stairs
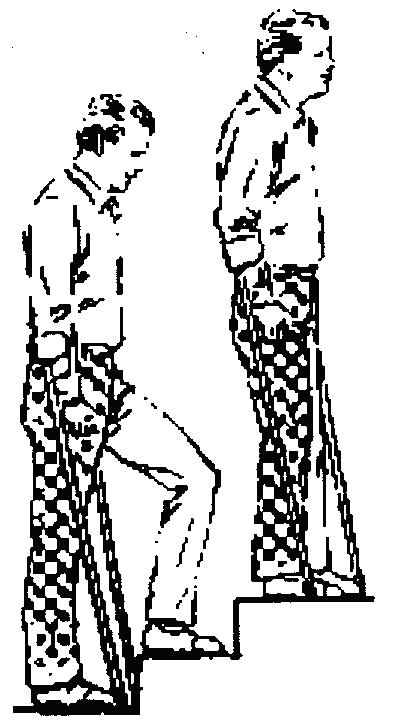 Before discharge home you will be shown how to go up and down stairs. Even if you live in a flat Before discharge home you will be shown how to go up and down stairs. Even if you live in a flat 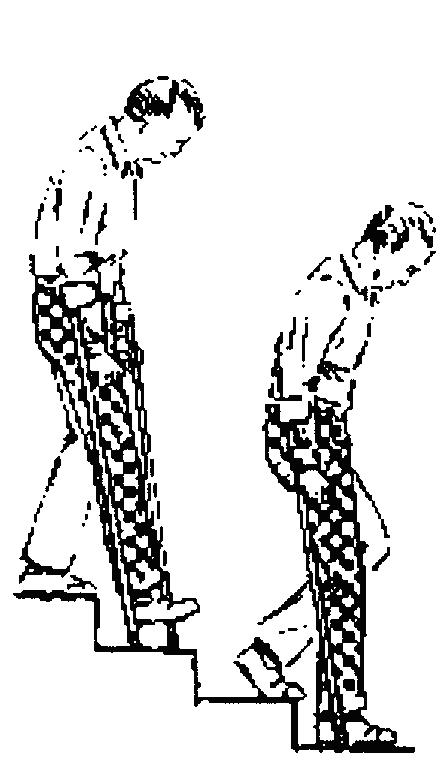
or a bungalow, it is a good idea to practice while in hospital, as it allows you to go out and visit
friends, without worrying about managing kerbs or steps.
Going up - Move your good leg first, then your new knee and sticks
Going down - Sticks first, then new knee followed by good leg
Getting in and out of the car
 When getting into a car, have it parked away from the kerb so that you do not have to stoop too low to get in. When getting into a car, have it parked away from the kerb so that you do not have to stoop too low to get in.
Have the seat adjusted as far back as it will go and recline the backrest. Sit sideways on the seat first, and then keeping your operated knee straight, slowly swing your legs into the car so that you are facing the front. A glossy magazine or plastic bag on the seat helps you turn in the seat.
Avoid bending your knee more than 90 degrees or raising your knee higher than your hip. If the seat is too low, you may need a cushion or pillow to raise you a little.
Prevention of infection
If at any time after surgery you develop an infection, you need to visit your family doctor. For example if you develop a urine infection, tooth or gum infection, infected cut or boil. He may decide you need a course of antibiotics. Viral infections like colds are not a problem.
Dental work can sometimes release bacteria into the bloodstream. Always tell your dentist that you have had a knee replacement. He may decide you need a course of antibiotics.
When Do I Return To Clinic?
Your first appointment is approximately 6 weeks after discharge from hospital. The ward staff will make this appointment for you before you are discharged from hospital. At this appointment you will be examined and given advice on the long-term management of your new knee.
Partners in Care
We want you to be our partner in care. Please try to help by:
· Providing full information on your health history and related matters
· Following the advice given to you
· Accepting responsibility if you refuse treatment or
· medical advice
· Taking reasonable care of your own property and respecting the property of other people in hospital
· Keeping appointments and giving adequate notice if unable to do so
· Switching off your mobile phone when in hospital
· Not smoking except in designated areas
· Ensuring reasonable and responsible behaviour by yourself and your visitors
· Please return any equipment when you have finished with it
If you have any questions, which are not answered by this booklet, then please dont hesitate to ask your Consultant or one of the nursing staff.
|