|
KNEE ARTHROSCOPY
Introduction
Because of the increased emphasis of physical fitness, knee injuries are becoming more common not only in athletes, but also in the general population.
Arthroscopy is the examination of the inside of the knee with a fibreoptic probe. It has become one of the most frequently 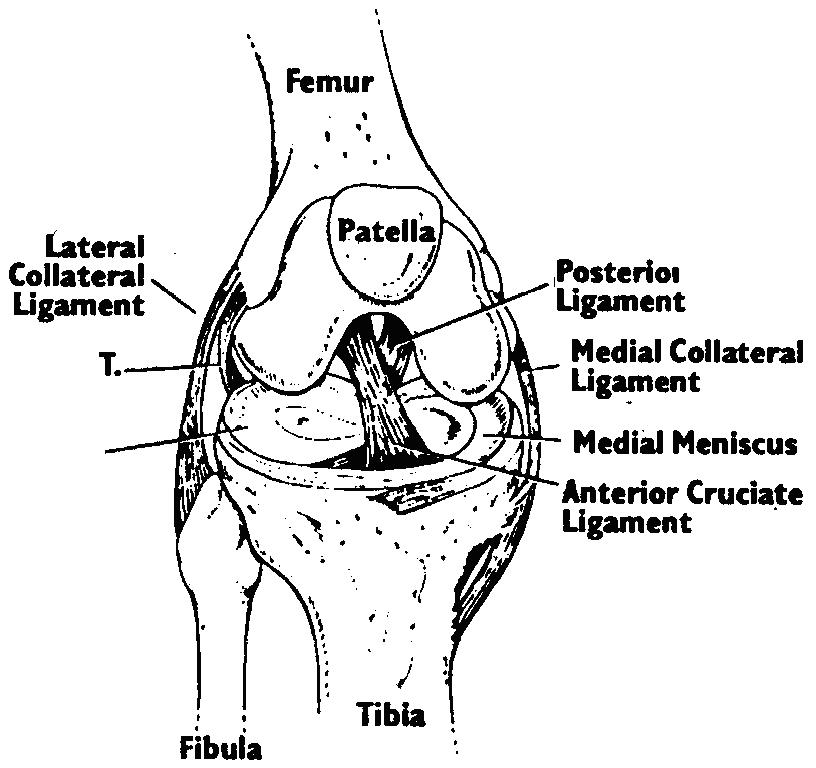
used and accurate tools for diagnosis and treatment of knee injuries. It is a surgical procedure which is performed as a day
patient.
Through a few small incisions the surgeon can insert the arthroscopy instruments into your knee. The arthroscope allows
the surgeon to see the entire knee joint, and some injuries or disorders, such as a cartilage tear, can be treated by removal
of the loose segment of the cartilage or, on occasion, repair.
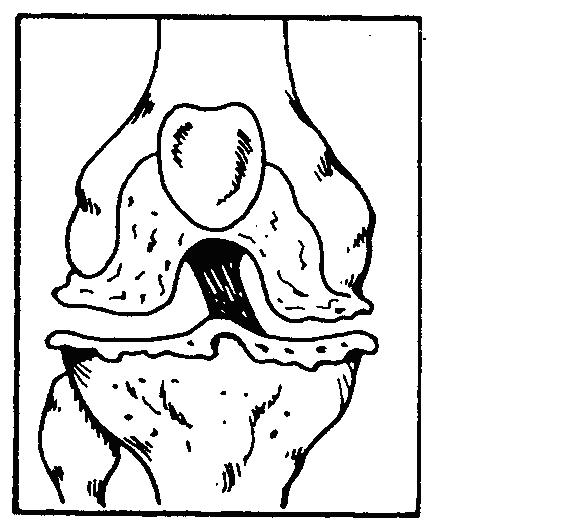
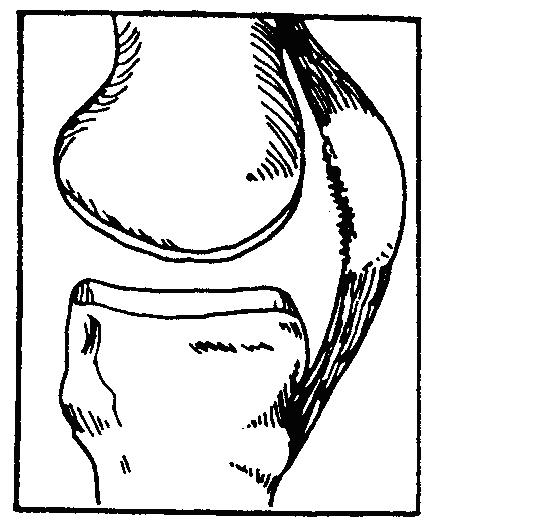
To help you understand your knee injury and the need for the arthroscopy it helps to know a little about the anatomy of a normal knee.
Hamstring
 Quadriceps Quadriceps
Gastrocnemium Tibia
Common Problems
Some of the more common knee problems include meniscus injuries, ligament injuries, degenerative disorders and patella derangements
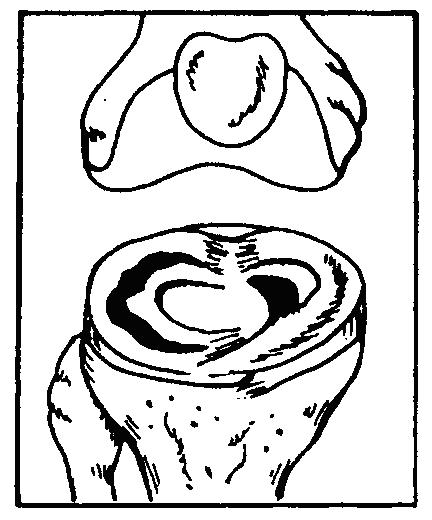
MENISCUS INJURIES - Menisci are the shock absorbing pads of cartilage in your knee. They may tear, split or fray
DEGENERATIVE DISORDERS - These are caused by changes in the joint surface cartilage. The cartilage may be rough or worn.

LIGAMENT INJURIES - Ligaments hold the bones together and stabilize your knee. Ligaments may tear completely or partially.
PATELLA DERANGEMENTS - The patella is the round bone in the front of your knee. It may be rough underneath or may not be in the correct
position.
Risks and Benefits of Arthroscopic Surgery
Just because your knee hurts it does not mean an arthroscopy is indicated. Your surgeon will question you and examine your knee. An ordinary X-ray is usually performed. A MRI scan can be helpful and, if normal, it is rare that an arthroscopy will be helpful to you.
If there are true mechanical features in your knee i.e. locking, giving way, jamming, it is more likely a remedial problem that can be identified and put right, such as a torn cartlidge.
Your surgeon will have given you some indication of the likely benefits of the procedure at consultation.
All operations under general anaesthetic have potential complications. Those associated with the anaesthetic are very rare in young people. Rarely are there severe local problems, which can include infections and which are less common than 1 in 1,000 patients who undergo arthroscopy. Perhaps 5-10% of patients, depending on the procedures undertaken, will have significant swelling that can take a while to go down. Venous thrombosis can occur but is uncommon.
In a sense, one of the most significant absences of benefit is that nothing is found that can be put right and you may continue with your symptoms. On rare occasions parts of the instruments can break and can usually be retrieved. On rare occasions the operation cannot be completed through the very small puncture wounds where the endoscope is inserted and an open incision may have to be undertaken. We cannot always advise you of this in advance and it is wise to consider that this is always a possibility. It does not mean that a major complication has occurred but it may slow your recovery down and you may have a little more pain and need physiotherapy and splintage or crutches for a slightly longer period.
The surgeons at Basford Consulting Rooms are trained and highly skilled in this procedure.
Pre-Operative Assessment
You will generally be called up to the hospital about one or two weeks before the proposed date of your operation. This allows doctors and nurses to check to see you are medically fit for the anaesthetic and operation. Fresh x-rays and blood tests may be taken.
You will be questioned about your current health and past medical, surgical or medication history. Particularly important things to tell the nurse or doctor about are:
* any heart problems
* asthma or any particular shortness of breath problems
* any bad reactions to a previous anaesthetic
This is an opportunity to tell the nurse of any worries or special needs when you return home after your operation. The operation should not be performed if there are any active infections. If any infections, including a bad cold occurs before your admission, please telephone the Hospital Admissions Officer or Basford Consulting Rooms.
You must bring all your current medicines prescribed by your doctor to the Assessment Clinic and on admission to the ward.
Smokers must stop prior to surgery to lessen the likelihood of a post-operative chest infection.
However, if you are young, fit and healthy, a pre-operative assessment is usually not required.
Pre-Operative Instructions
Most arthroscopic surgery of the knee is undertaken as a day patient procedure under general anaesthetic. Do not eat anything or drink anything after midnight, unless otherwise instructed by the doctor at the hospital.
What to bring to the Hospital
For day case surgery, personal toiletries may be brought in. Bring your routine medication with you and take routine medicines only as directed by the Anaesthetist or Surgeon.
Make arrangements to have a responsible adult available to drive you home after discharge following your day surgery. You will not be allowed to leave the hospital alone. You must not drive the same day as a general anaesthetic.
After admission to the Hospital
After you are admitted there will be further discussion with the day surgery nursing staff. You may be visited by a physiotherapist who will advise you of simple muscle bracing exercises. Any special post-operative exercises or rehabilitation needs will be indicated.
Before the procedure the Anaesthetist will talk to you and assess the most suitable form of anaesthetic, most often a general anaesthetic (being put to sleep). At any time please ask about the anaesthetic and post-operative analgesia. You may be given a pre-medication to make your wait less anxious.
You will be taken to the operating theatre on a trolley or bed. After the procedure there will be a light dressing on the knee.
After your Operation
You will be observed and monitored for a short period in the Recovery Bay area which is close to the theatre. You may have a small drip in a vein which will be removed later on the Ward. Once you are breathing comfortably you will be allowed back in the ward to the Day Unit. You may remain in the Day Unit for an hour or so but this may vary according to the surgical procedure and the type of anaesthesia. Various checks on your blood pressure etc will be taken and your circulation, sensation and comfort will be assessed.
Before discharge you will be asked to stand and walk. You may feel tired and dizzy but this is a normal reaction following anaesthesia. The nurse will be there to assist you and advise. The nursing staff are trained to assess whether you are safe to go home. If you cannot perform a straight leg raise, i.e. have good limb control, the nursing staff may advise a splint and they or the physiotherapists will assess the need for walking aids (crutches).
Analgesics (medication) for pain will be provided for you to take if you have severe pain. You should not drink alcohol when you are taking the medication. As your recovery progresses Paracetamol should be sufficient.
Discharge Instructions
You may feel a little drowsy for 24 or 48 hours and you should have someone at home. You must put as much weight on the operated leg as has been advised by your surgeon or physiotherapist. Keep your bandages clean and dry and do not remove them until you return to the clinic or as instructed by your surgeon. The dressing should not come into contact with water. If you bathe, cover the bandaged leg with a plastic bag, fastening securely beyond the upper edge of the bandage or dressing, with tape. There may be a small amount of pink or red drainage through the outer surface of the dressing, which is normal. If this increases in amount over a 12 hour period you should report this to the Day Unit or to your General Practitioner.
Elevate the operated leg, if possible, in the first 48 hours and an application of an ice pack will also help reduce any pain and swelling. When sleeping a pillow should be used to keep your leg up. Elevation in the first few days is a precaution that can prevent post-operative complications.
Exercises
These are general exercises and you may be advised to modify them by the physiotherapist or your surgeon, according to the different circumstances. You must practice these exercises because if you do not, the knee may feel weak and there may be a sensation of giving way.
QUADRICEPS SET 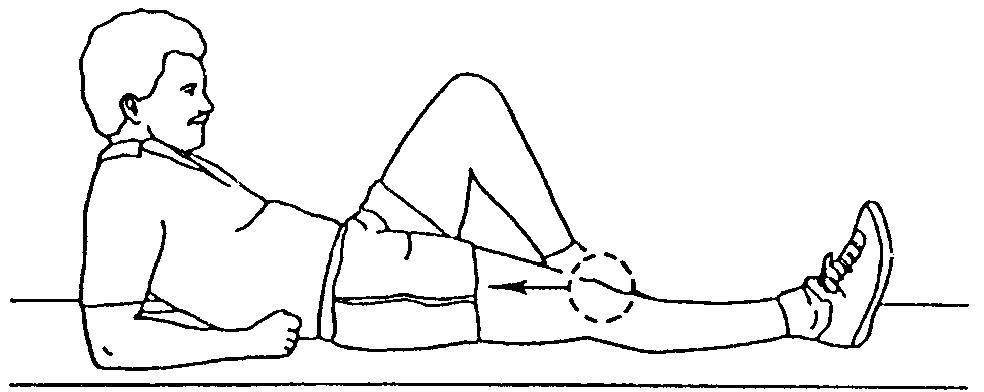
The quadricep is the front of knee muscle. Tighten this muscle to make your kneecap move. Hold this contraction for 5 counts and then relax. This exercise is done with the leg straight and can be performed standing, sitting, or lying down.
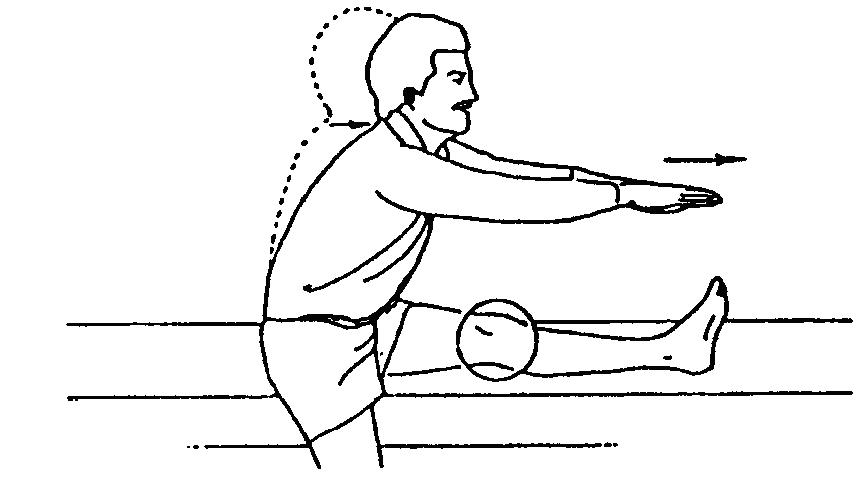
HAMSTRING STRETCH
Straighten supported leg with thee opposite leg off the side. Slowly lean forward until you feel a stretch at the back of your knee. Hold stretch for 10 counts. Do this with chin up, back straight, and without bouncing.
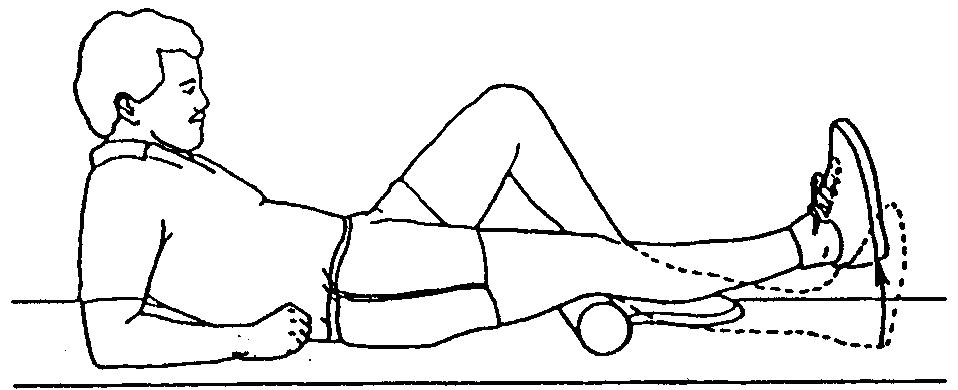 TERMINAL KNEE EXTENSION TERMINAL KNEE EXTENSION
Lie on your back and place a towel roll under your knee allowing your knees to bend slightly. Lift heel in order to straighten your leg. Hold for a count of 5 and then relax.
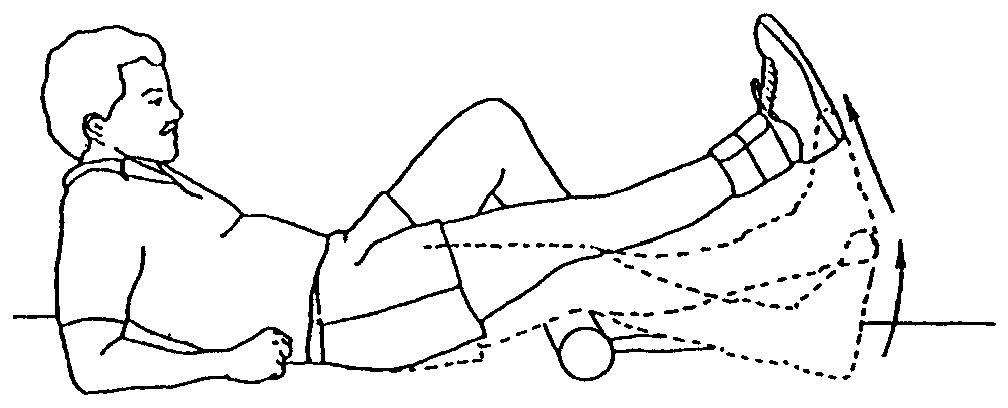 STRAIGHT LEG RAISE WITH HEEL LIFT STRAIGHT LEG RAISE WITH HEEL LIFT
Lie on your back and place a towel roll under your knee allowing it to bend slightly. Bend your opposite knee to protect your low back. Lift your heel in order to straighten your leg. Once the leg is as straight as possible, lift the entire leg to height of opposite knee. Hold for 3-5 counts and relax.
To add resistance, secure weight on top of thigh. Begin with 1-2 Lbs and gradually increase.The physiotherapist will advise you with regard to this.
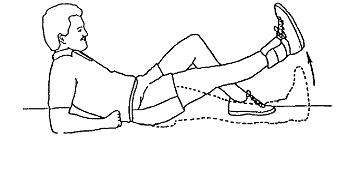 STRAIGHT LEG RAISE STRAIGHT LEG RAISE
Lie on your back with opposite knee bent. Tighten the knee muscle performing a quad set. Lift your leg straight up slightly lower than your bent knee and hold 3-5 counts. The knee should be straight throughout the lift. Relax leg between each lift.
To add resistance, secure weight on ankle. Begin with 1-2 lbs and gradually increase.
Rest 30 seconds to 1 minute between each set of 10.
CONCERNED? - CONTACT US
Contact the Day Unit nurse or your General Practitioner if the following occurs:
* swelling
* tingling, (pain or numbness in your toes which is not relieved by elevating
your foot for a period of one hour)
* foul smell with discharge or drainage from your bandage
* mouth temperature above 38.5ºC or 101 .3ºF
* pain in the operated leg which is not relieved by test, leg elevation or
pain medication
|